Endoscopic Anterior Cervical Discectomy Without Fusion Through a Two Millimeter Opening
Source: ISASS Annual Meeting, May 2014.
INTRODUCTION
The anatomical and biomechanical characteristics of the degenerative cervical intervertebral disc may make it more prone to instability after conventional discectomy. The addition of fusion, with or without instrumentation, is a logical solution to such a problem; however, it produces long term overload of adjacent cervical levels which in turn, increases the incidence of disc degeneration and/or the development of disc herniations. The following abstract describes the results of an anterior cervical focalized discectomy through a tiny "nano"- approach.
METHODS
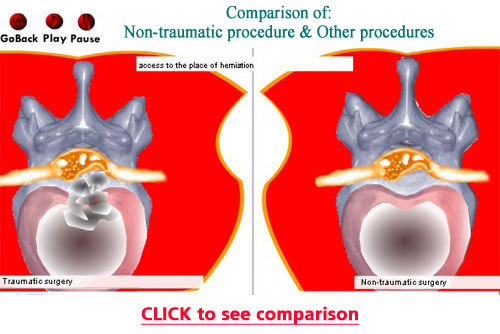
In 2011 and 2012, 21 patients were treated. 66% were males, 34% were women, from 23 to 73 years old, with an average of 50 years old. Only 29% of the cases presented with pure disc herniations and 71% were accompanied by osteophytes, all with radiculopathy and without myelopathy. The average follow-up was 8 wks. Technique: Under general anesthesia, a 2 mm-skin opening is made and a guide wire is introduced medial to the vessel and lateral to the esophagus. Dilating cannulas (2 mm) are introduced. Using fluoroscopy and endoscopic visualization, focal discectomy is manually performed with micro-instruments targeting the causative pathology.
RESULTS
The success rate was 95% following the MacNab criteria. Excellent 47.5% (n=10), Good 47.5% (n=10), Fair 5% (n=1) and Poor none. There was one case of negative pressure pulmonary hypertension, a complication unrelated to the surgery itself. This was resolved without sequelae.
CONCLUSIONS
Focal anterior cervical discectomy without fusion through a "nano" approach is a very effective and safe way to treat cervical disc herniations with or without osteophytic components. The limited disc resection does not produce instability or the need for fusion and preserves underlying bio-mechanical function.
|